
It’s not every day that you witness the moment the lives of hundreds of thousands of families tumble out of control. But that’s what happened while I sat in traffic with my wife and eight-month old baby while we were on our way to Makati Medical Center for my daughter’s scheduled check-up.
Our Grab driver’s radio was tuned into one of the many animated news talk shows broadcast in Manila, the Philippines’ heaving swirl of a capitol city. The announcer was reading from the news summary that was read at the top and bottom of every hour. There was news about a new vaccine that had been administered to over eight-hundred thousand children in what is referred to as the National Capitol Region (NCR).
From April 2016 until November 2017, school children were inoculated against dengue using a groundbreaking dengue vaccine from Sanofi Pasteur called Dengvaxia. It was supposed to bestow life-long immunity to the virus that causes the disease. Instead, it became a proxy for all the misfortune that falls on the disenfranchised.
In a deliberately phrased statement from the French pharmaceutical giant, families whose children had been injected with their vaccine were informed
For those not previously infected by dengue virus, however, the analysis found that in the longer term, more cases of severe disease could occur following vaccination upon a subsequent dengue infection… Vaccination should only be recommended when the potential benefits outweigh the potential risks (in countries with high burden of dengue disease). For individuals who have not been previously infected by dengue virus, vaccination should not be recommended.
The reaction was swift and savage. For many parents, it was viewed as a death sentence for their children.
As a prominent doctor in the Philippines later observed, now the children would be forced to live with the possibility of contracting severe dengue for the rest of their lives. Considering the fact that, if not treated properly, up to 20% of severe dengue cases are fatal. He was also implying that hundreds of children would die in the coming years. He had the tact to not say it directly.
As the announcers commented on the news and played excerpts of politicians expressing a healthy dose of self-serving indignation, there were already hints at the uncontrollable swirl of forces that would remain unresolved over a half-decade later. Fear, grandstanding, elitism, opportunism would drive the narrative forward and a long history of indignities would serve as the fuel.
If you enjoy the content we create and would like to support us, please consider becoming a patron on Patreon! By joining our community, you’ll gain access to exclusive perks such as early access to our latest content, behind-the-scenes updates, and the ability to submit questions and suggest topics for us to cover. Your support will enable us to continue creating high-quality content and reach a wider audience.
Join us on Patreon today and let’s work together to create more amazing content! https://www.patreon.com/ScientificInquirer
A Cruel Disease
Sanofi Pasteur’s dengue vaccine, Dengvaxia, was supposed to make life easier for the children and parents in the Philippines by removing a major source of morbidity among children. For years, dengue infections had been on the rise, and there was legitimate concern that the illness would result in a serious economic and public health burden.
For President Benigno “Ninoy” Aquino III, the vaccination campaign should have been one of his parting gifts to his people and a boon to his legacy. Under his guidance, the Philippines kicked out of its lethargy and shed the monicker “Sick man of Asia”. Economic growth had become amongst the top in Asia. Foreign investors – long wary of the topsy-turvey climate in the island nation – now viewed the country as a favorable place to invest. After the tumultuous presidencies of Joseph Estrada and Gloria Macapagal Arroyo before him, Aquino provided a much needed period of stability and predictability.
This trial is a cautionary tale for investigators designing future dengue vaccine efficacy trials.
Scott Halstead.
During his term in office, Aquino watched as year after year, dengue infections and subsequent mortality outpaced most other communicable diseases. In 2011, Dengue accounted for 639 deaths and 118,868 infections. The following year, 872 and 178,643 infections. In 2014, the year before the Aquino administration set its Dengvaxia strategy in motion, the Philippines had 425 fatalities from 113,485 infections. For many public health officials and epidemiologists, dengue represented a pressing concern that threatened the country on a very basic level – its people.

The disease is considered hyperendemic in the Philippines, which means that the disease is present in high levels and has become deeply established within the population. The Philippines is one of the countries with the highest incidence of dengue in the world, with an estimated 200,000 to 400,000 cases reported each year. Dengue is endemic in all regions of the Philippines, with varying levels of transmission intensity and disease burden across different regions.
Because of the prevalence of the disease in the country, most children under 9 years of age have been infected at least once. Typically, the first infections range from being asymptomatic to presenting mild symptoms. It is upon a second infection that bad things tend to happen. Symptoms can be much more severe, often leading to dengue hemorrhagic fever, a considerably more dangerous. Symptoms tend to include severe headache, eye pain, and muscle and joint pain, unusual bleeding from the gums or nose, or blood in urine or stool, and skin rash. Hospitalization is necessary at this point.
On some occasions DHF can descend further into a condition called dengue shock syndrome which culminates in the body’s organs shutting down due to reduced blood flow due to narrowing of blood vessels.
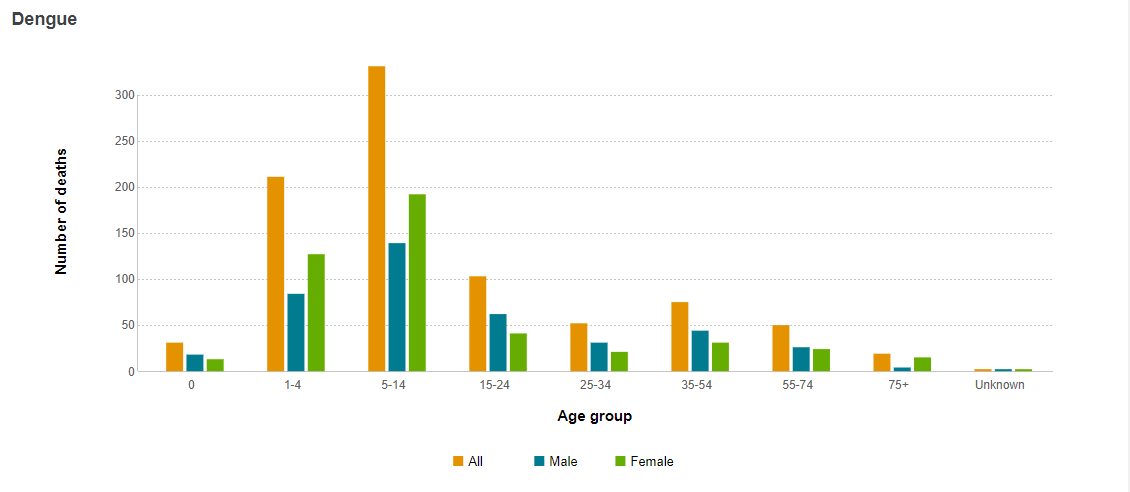
There is an insidious aspect to the disease in the Philippines that makes it hit harder than most. Whereas in countries like Mexico and Brazil the disease tends to cause fatality among adults over 30 years of age. Dengue in the Philippines strikes young children the hardest, as can be seen in the following graph.
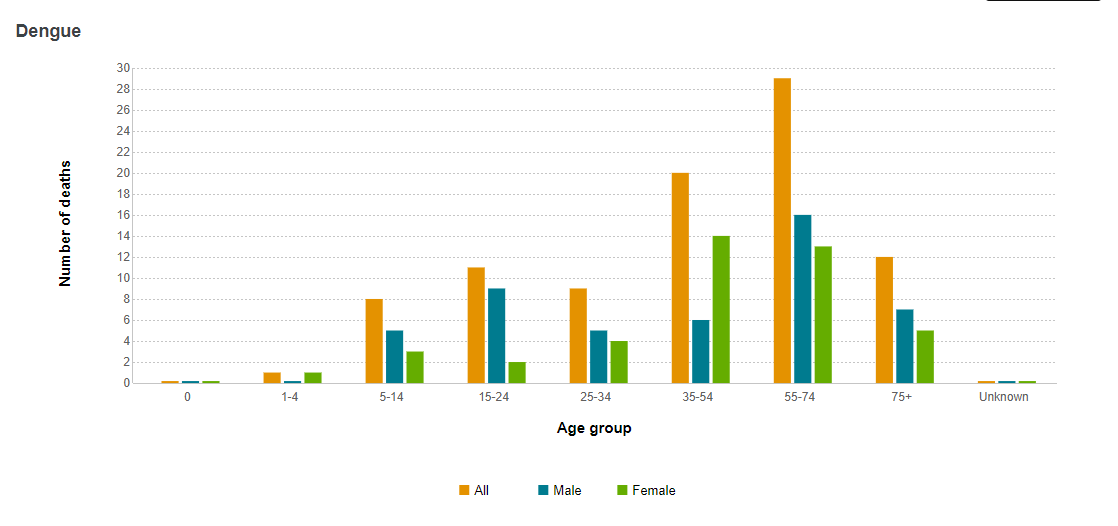
In stark contrast to dengue in the Philippines, Mexico sees most of its infections among adults.
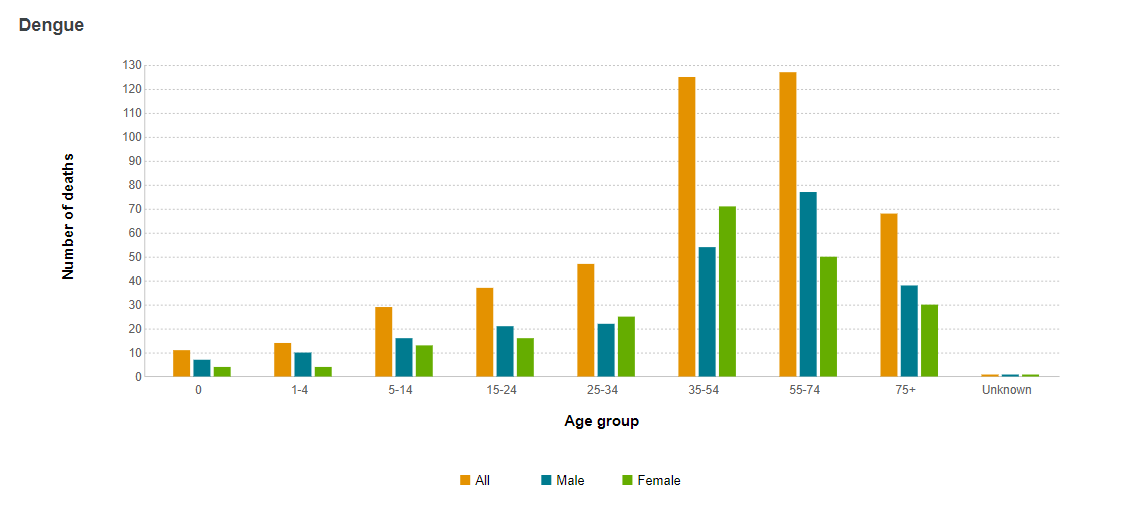
Dengue in Brazil also affects adults much more than children.
If a safe and effective vaccine were available that promised to reduce infections and fatalities by more than half, what public health official or policy maker wouldn’t jump at the chance of providing it. Who can blame them?
The Rocky Road Towards a Partially Effective Vaccine: Safety and Efficacy Questions
Sanofi Pasteur recognized the devastation dengue was causing worldwide and identified it as an opportunity. Dengue, a disease primarily affecting tropical countries (also known as the Global South), had been regarded as a neglected disease. However, as its spread continued, surpassing malaria in terms of infections and fatalities, Sanofi began envisioning it as a potential blockbuster drug.
The company invested considerable resources into developing a dengue vaccine, although the development of the vaccine predated their involvement. The technology used in the vaccine originated at the St. Louis University Health and Sciences Center. The Chambers Laboratory developed a method to generate chimeric yellow fever/Japanese encephalitis (YF/JE) viruses from cDNA templates encoding structural proteins.
This “chimeric” approach allowed for the creation of a live, attenuated vaccine using the backbone of yellow fever, which later served as the basis for a dengue vaccine developed by the British biotech firm Acambis, Inc., a major supplier of smallpox vaccines to the United States. They were working on several other vaccines for Japanese Encephalitis, dengue, and West Nile virus in collaboration with Sanofi.
Eventually, the French pharmaceutical company decided to acquire Acambis, having set its sights on the firm’s vaccine platform.
The Dengvaxia vaccine, developed by Acambis and Sanofi, is a live attenuated tetravalent vaccine that uses chimeras consisting of structural pre-membrane and envelope genes from all four dengue subtypes, subsequently mixed with non-structural genes of a weakened version of yellow fever.
By combining all of the subtypes into a single vaccine, researchers hoped it would provide equal, long-lasting protection against all four circulating dengue strains. Theoretically, it could eliminate the issue vaccines face when strains rotate in and out of circulation, a problem that continues to plague influenza vaccines.
Studying dengue has proven tricky for scientists due to the lack of a good animal model that reflects human infections. Despite this, researchers didn’t stop trying to overcome this hurdle. After successful in vitro studies, Dengvaxia was tested on Rhesus and cynomolgus macaques. The vaccine effectively protected them six months after the initial vaccination, although this proved to be misleading.
Dengvaxia’s clinical trials began with Phase I, first conducted in the United States with sero-negative individuals, then in the Philippines and Mexico where dengue is endemic. According to those studies, the vaccine was safe to take and caused no fatalities. However, this marked the end of smooth sailing for Sanofi.
In Phase 2b testing, the vaccine was administered to a larger population to assess its safety and efficacy. Sanofi Pasteur reported an overall efficacy of around 60%, but it was significantly lower in certain populations. For example, the vaccine’s efficacy was only about 30% in individuals who had never been exposed to the dengue virus before.
Furthermore, during Phase 2 testing, it was discovered that the vaccine could potentially exacerbate the disease in some individuals who had not been previously exposed to the dengue virus. This was due to a phenomenon known as antibody-dependent enhancement (ADE), where the vaccine could increase the severity of the disease in some individuals instead of protecting them from it.
At this stage, other scientists began expressing concerns about the vaccine’s efficacy. Prominent among them was Scott Halstead, one of the world’s leading dengue researchers. In a letter written and published in The Lancet, he warned,
This trial is a cautionary tale for investigators designing future dengue vaccine efficacy trials. A much larger group of vaccinees should have been studied serologically than was the case here. When flavivirus-immune populations are given complex dengue vaccines, the postvaccination efficacy of DENV vaccines and the serological responses can only be interpreted in the context of prevaccination immune status.
In other words, it was crucial that children receiving the vaccine were tested beforehand to determine whether they had been previously infected or not. This warning proved to be prescient.
Despite the challenges, Sanofi proceeded with Dengvaxia into Phase III trials. The results were not much better.
Dengvaxia’s Phase 3 trials were designed to further assess the safety and efficacy of the vaccine on a larger scale, and to confirm the findings of Phase 2. These trials involved thousands of participants across multiple countries over several years.
The Phase 3 trials were divided into three main studies, each with slightly different objectives and patient populations. The first study, CYD14, was conducted in Southeast Asia and Latin America and involved over 10,000 participants aged 2 to 14. The second study, CYD15, focused on individuals aged 9 to 16 and was conducted in Latin America and the Caribbean. The third study, CYD57, was conducted in five Asian countries and involved over 20,000 participants aged 2 to 45.
Overall, the Phase 3 trials found that Dengvaxia was moderately effective in preventing dengue fever, but its efficacy varied depending on the individual’s age and prior exposure to the virus. In individuals who had never been exposed to the dengue virus before, the vaccine’s efficacy was lower than in those who had previously been infected. Furthermore, the trials confirmed the potential risk of severe dengue disease in individuals who had not previously been exposed to the virus, a finding echoed in the Phase 2 trials.
The most contentious part of the Phase 3 trials was the risk of severe dengue among individuals without prior infection, brought about by the then-controversial idea of antibody-dependent enhancement (ADE). ADE is a phenomenon where antibodies generated in response to a viral infection or a vaccine can actually enhance the severity of the disease when the individual is subsequently infected with a related virus. ADE occurs when the antibodies produced in response to the initial infection or vaccination do not fully neutralize the virus, but instead bind to it and facilitate its entry into immune cells, leading to more severe disease. This phenomenon was first proposed by Scott Halstead and was only confirmed recently.
For Halstead, the Phase 3 data confirmed ADE’s role in severe dengue onset. In a perspective piece published in The Journal of Infectious Diseases, he explained how ADE was responsible:
The combination of poor protection against DENV infection of individuals with circulating DENV antibodies (monotypic immune equivalents) satisfies the known preconditions for antibody enhancement of infection.
He further explained,
When a vaccine has the potential to sensitize a recipient to immune enhancement, a classical efficacy calculation is not relevant. In the vaccine group, seronegative individuals may be converted by vaccine to so-called monotypic immune equivalents who experience disease hospitalizations during breakthrough primary DENV infections, whereas hospitalizations in the placebo groups occur during secondary DENV infections... These rates cannot be compared.
Despite these uncertainties, Sanofi continued to push for Dengvaxia’s approval. The company received a major boost when the World Health Organization fully and unconditionally endorsed the vaccine. Capitalizing on this endorsement, the pharmaceutical giant stated,
These WHO SAGE recommendations further validate the scientific and medical value of Dengvaxia and send a clear message to endemic countries about the strong public health benefit to be gained by introducing the dengue vaccine in integrated disease management efforts to combat their dengue burden.
A Fierce Biotech article titled “Sanofi’s Dengvaxia gets a boost from WHO recommendation” emphasized the importance of receiving WHO’s blessing, saying,
WHO’s endorsement could prove a key boost for a vaccine that’s still in the early stages of a high-stakes rollout... The announcement also comes at a pivotal point for Sanofi and CEO Olivier Brandicourt, who is working to build revenues and reshape the company as competition and pricing pressure eat away at diabetes revenues. In February, the pharma eliminated 500 positions in its native France following Brandicourt’s €1.5 billion cost-cutting initiative announced in November.
It’s difficult to say how quickly countries would have adopted the vaccine based solely on its own merit. The World Health Organization’s recommendation paved the way for countries to adopt Dengvaxia and build immunization programs around it. Unfortunately, the Philippines was the only country that fully committed to this initiative.
SANOFI’S ROSE TINTED GLASSES
Sanofi desperately needed a blockbuster. Despite being one of the world’s most prestigious pharmaceutical companies – especially its vaccine division, which was founded by Louis Pasteur and acquired by Sanofi over a century later – fortune had been unkind to the company. Even before Dengvaxia hit the market in 2016, a series of setbacks and disappointments haunted the company. It was relentless.
In 2011, the company received its first significant setback when it lost exclusivity on a number of its drugs, including Lovenox, an anticoagulant drug used to prevent and treat deep vein thrombosis and pulmonary embolism; Plavix, an antiplatelet drug used to reduce the risk of heart attack and stroke in patients with cardiovascular disease; Avapro, used to treat high blood pressure (hypertension) and help protect the kidneys from damage due to diabetes; and Ambien CR, a prescription sleep aid used to treat insomnia. The loss of exclusivity, designed to keep prices down by allowing other companies to manufacture generic versions of the drug, resulted in losses of €553 million on the following year’s balance sheet.
While the company struggled to make up for the 2011-2012 shortfall, it received a series of setbacks in 2013. After a major scandal in China involving GlaxoSmithKline, Beijing cracked down on Western pharmaceutical companies’ sales practices, causing sales and stock prices of foreign companies to drop. Additionally, the US Food and Drug Administration (FDA) rejected Sanofi’s initial application for approval for its multiple sclerosis drug, Lemtrada, citing concerns about the design of the clinical trials and the need for more data. (The FDA eventually approved the drug in November 2014, but with a boxed warning and a Risk Evaluation and Mitigation Strategy (REMS) program to monitor the drug’s safety.) The miserable year saw Sanofi cutting its earnings forecast from the second quarter onwards.
During its Q3 earnings call, then-chief executive Chris Viehbacher told reporters that the problems encountered during the quarter were largely one-offs that the company had now put behind it. “We’re confident about being able to get back to growth in the fourth quarter,” he said, remaining optimistic despite the company’s setbacks.
The company remained bullish on Dengvaxia’s potential, even in the face of disappointing Phase 2b trial results that saw efficacy dipping to 30% in some populations. In its 2013 Q4 Earnings Call, Elias Adam Zerhouni painted a bright picture of the vaccine’s performance, presenting a glass-half-full outlook.
The first-in-class dengue vaccine, which is being developed by Sanofi Pasteur, is addressing a growing global threat,” he said. “It is an ambitious development program undertaken by Sanofi Pasteur. The Phase IIb results in 4,000 children observed efficacy against 3 of the 4 serotypes involved. More importantly, it was the first time that a vaccine approach was demonstrated to be safe in dengue, and we're eagerly awaiting the results of the Phase III studies, the 2 large-scale studies in Asia and Latin America involving 31,000 children and adolescents, which we'll hear about in the second half of 2014.
He predicted peak forecasts of $200 million a year but indicated that this was a conservative estimate.
Just how bullish was the company on Dengvaxia and how much did they have at stake? Two things stand out. Both represented how much the company needed Dengvaxia to be the first to hit the market. Being the first mover in a space provided the opportunity to establish strong brand recognition, secure key distribution channels, develop customer loyalty, and gain an uncontested market share. By introducing a novel product, first-movers can set industry standards and control the direction of market development.
During the Q3 2013 conference call, Zerhouni hinted at a special unit within Sanofi Pasteur that existed solely to bring the world’s first dengue vaccine to market and ensure its wide adoption.
“I'm looking at the dengue vaccine, and I see peak sales forecasts of $200 million,” he said. “We are busy recruiting a lot of people inside the company and bringing expertise into some of these areas. We certainly have it in dengue."
The unit even had a name: The Dengue Company.
In a 2015 interview, Guillaume Leroy described the special unit’s purpose,
Due to the nature of the market, the product being created had to be an incremental innovation and a breakthrough. A first mover advantage was crucial in the vaccine industry. One example is the MSD Gardasil vaccine, which made 2 billion dollars in sales in its first year. It is estimated that the demand for the dengue vaccine will be 2.5 billion vaccine doses after the first 5 years of introduction. As a result, Sanofi took action to reduce the time for the vaccine to enter the market by having the industrial capacity to manufacture vaccines built alongside the development of the vaccine to reduce the time to market. ‘Our industrial capacity is our main tool to conquer the market.’ To reduce time and production, a separate internal structure called the Dengue Company was created that consisted of a core group of employees that had roles dedicated to dengue vaccine development, production, and marketing.
If there was one sign that spoke to Sanofi’s determination to bring Dengvaxia to market and get it into the arms of people around the world, it was this:
In an unusually aggressive move, the company decided to custom build a factory in Neuville-sur-Saone, France, just for the production of Dengvaxia. By July of 2013, a full year before Phase 3 results from two clinical trials were reported and two years before being approved by any sanctioning body, Sanofi started production of Dengvaxia in earnest. They acted with the sole purpose of winning the race to the market.

When a new CEO, Olivier Brandicourt, rose to the helm, he brought an aggressive vision for the struggling company that revolved around three elements: diabetes, cardiovascular treatments, and vaccines. At the heart of that third category sat Dengvaxia, the billion-dollar golden goose. There was no way Sanofi’s executives, board members, and investors would let it go down without a fight. Armed with the WHO’s tacit endorsement, Sanofi officials focused their efforts on finding customers and the ultimate prize, the promise of a mass vaccination program.

GRADING DENGVAXIA
So, what kind of vaccine had Sanofi sold to governments eager to roll out a new weapon against dengue fever? If you consider all of the published studies, distributed guidance, and qualified endorsements, you are left with an uncertain feeling. You might conclude that Dengvaxia is a decent (not great) vaccine that isn’t very effective. After a while, it’s hard to determine where the vaccine stands on the spectrum of good or bad. Fortunately, the U.S. Centers for Disease Control conducted its own analysis of Dengvaxia that paints a clear picture of how it compares to a hypothetical drug.
The CDC’s Grade Analysis of Dengvaxia provides the clearest picture of how the vaccine had been approved, endorsed by the World Health Organization, and sold and marketed by Sanofi Pasteur.
This Figure 25 demonstrates how a prior infection with Dengue significantly impacts disease progression. For children who have already been infected with dengue at some point before being inoculated (seropositive), Dengvaxia performs well. Five out of six of the data points sit well within the “Favors Dengvaxia” zone. Only among 2 to 8-year-olds does it drift toward favoring the placebo.
On the other hand, the results among children who had never been infected with Dengue are almost all negative and actually favor the control. That means that more children who had been vaccinated ended up with severe dengue than those who received the placebo, e.g., “Favors Control”. Dengvaxia’s performance is plain to see.
The Hazard Ratio values provide a numerical sense of Dengvaxia’s effectiveness. It is used to determine the effect of a treatment. A value of 1 is considered the boundary between a favorable treatment and a hazardous one. Anything less than 1 is considered good. The smaller the number, the more effective the vaccine. On the flip side, anything greater than 1 is considered a cause for concern. The higher the value, the less effective the vaccine.
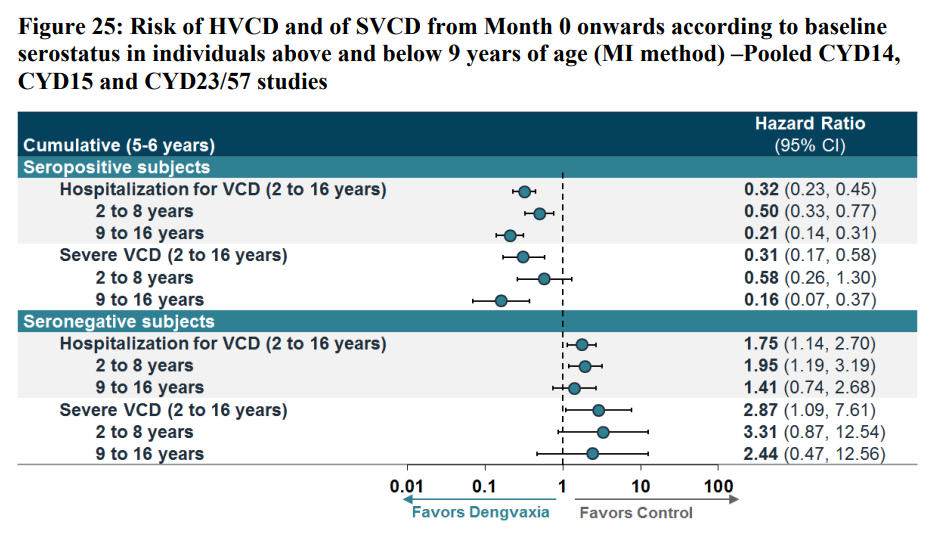
According to Figure 25, Dengvaxia performs decently among most seropositive individuals but really goes off the rails for seronegative children. Not only that, the Hazard Ratios are consistently over 1. The highest value is 3.31, meaning children who receive a shot of Dengvaxia are 3.31 times more likely to die than those who received a placebo.
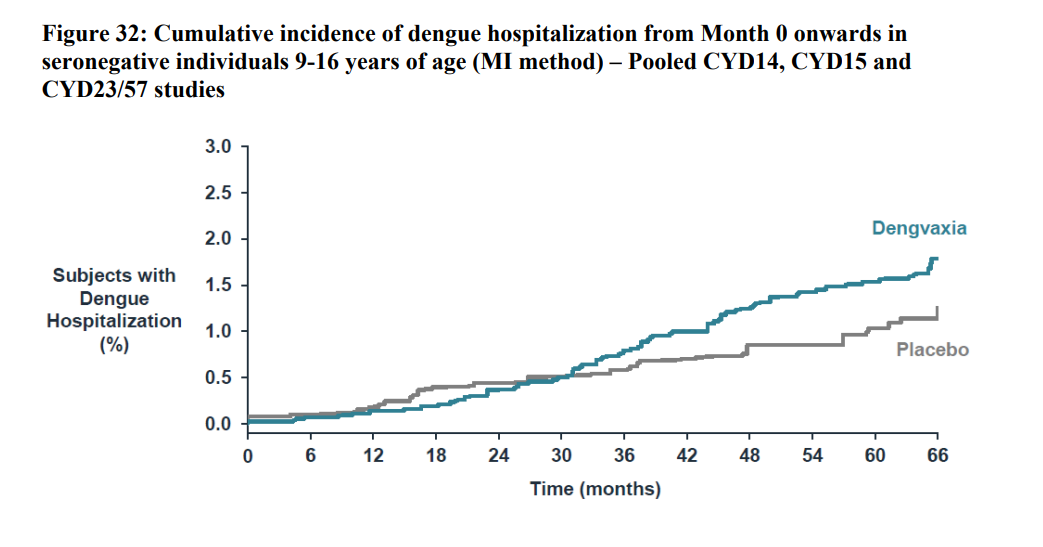
Figure 32 further reinforces the fact that children between 9-16 years old without prior infection are more likely to develop severe dengue and be hospitalized compared to children who were not vaccinated at all. After starting at the same position on the graph, the blue line diverges quite decisively from the gray placebo line.
The situation becomes even worse for severe dengue cases without hospitalization.
In Figure 32, the higher the line, the worse the performance. The divergence between Dengvaxia and the placebo is quite drastic. This applies to the 9 to 16 year olds, the group that was cleared by Sanofi and the WHO for vaccination.
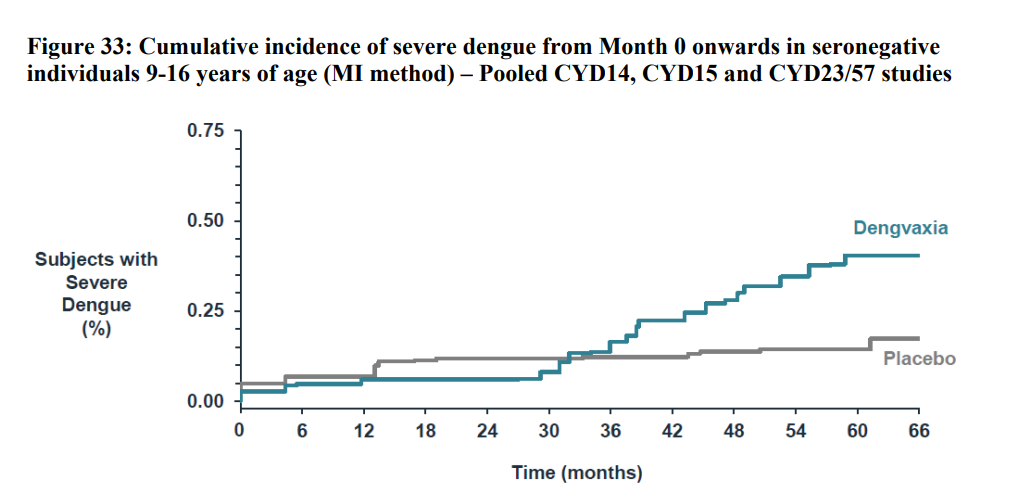
In Figure 33, the data for Dengvaxia’s effectiveness is just as bad. The difference between the vaccine and the placebo can’t be ignored.
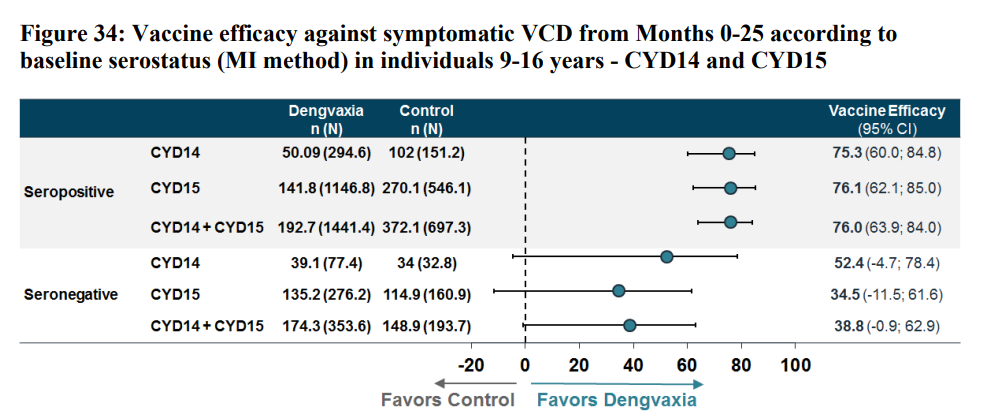
For comparison, look at Figure 34, where the vaccine is effective. For children who had a previous dengue infection, the data points are so far to the right that the efficacy is well into the mid-80s. Meanwhile, the efficacy numbers for those who were seronegative come in at 38.8 when CYD14 and 15 are combined.
This was the vaccine that Sanofi had greenlit and that had received the World Health Organization’s unequivocal seal of approval. This was the vaccine that was administered to nearly a million school children in the Philippines.
Roll Out Questions
In April 2016, parents of school children in regions of Central Luzon received notice that their children would be receiving a vaccine to protect against the virus responsible for dengue fever. With the school year having ended, thousands of children would need to make special trips back to school during their summer breaks. It was important though, and most, if not all, parents went out of their way to ensure their kids received the protective jabs. They had no reason to doubt the government’s decision to commit so enthusiastically to the new vaccine. On some matters, the social contract between citizens and the government in the Philippines proved resilient, even in the face of countless scandals and farces.
If Dengvaxia’s mediocre clinical trial results caused hand wringing at Sanofi, the company certainly put on a brave face. They had a lot to lose. Over the past two decades, they had invested heavily in their determined march towards first-mover advantage.
We went to her [Sec. Jeanette Gain] and said, ‘this is something that we should be concerned about. We should start asking, why are they recommending this vaccine only for nine-year-olds and older because biologically it doesn’t make sense.
Final results from Phase 3 clinical trials contained enough red flags to attract the attention of several doctors and scientists experienced in dealing with dengue. In the Philippines, Leonila and Antonio Dans were perhaps the most vocal and visible critics. Meanwhile, experts outside the country also weighed in. Notably, Scott Halstead reiterated his concern that the danger of antibody-dependent enhancement needed to be taken into consideration.
On April 12-14, 2016, nearly two weeks after the Philippines plunged head-first into its immunization campaign, the WHO SAGE Working Group met to issue its recommendation for Dengvaxia. Yet, even after endorsing the vaccine, SAGE also reported its concerns about the Phase 3 trial data.
In those children vaccinated at ages 2–5 years in Asia, a statistically significant increased risk of hospitalized dengue was seen in vaccine recipients in the third year after the first dose, though this dissipated in years 4 and 5. The biologic mechanism behind this increased risk is currently not understood but may be related to naïve vaccine serostatus and/or age. A significant increase in hospitalizations was not seen in those older than 5 years. No other safety signal has been identified.
Ultimately, the group parsed words by stating that countries should decide for themselves.
Decisions about introduction require careful assessment at the country level, including consideration of local priorities, national and subnational dengue epidemiology, predicted impact, cost-effectiveness with country-specific hospitalization rates and costs, affordability, and budget impact.
They offered guidance regarding who should be vaccinated, saying,
Because of the safety signal of increased risk of hospitalized and severe dengue identified in the 2–5 year age group, CYD-TDV is not recommended for use in children under 9 years of age, consistent with current labeling. The target age for routine vaccination should be defined by each country based on an assessment of dengue endemicity and programmatic feasibility of targeting particular age groups. For the most highly endemic settings (e.g., seroprevalence at 9 years of age of approximately >90%), 9 years of age is projected to maximize impact. In settings with seroprevalence at 9 years below 90% (but above 50%), 11–14 years of age may be preferable.
To Leonila Dans, none of it made sense. The fact that the vaccine was harmful to 2-5 year olds was a significant signal and not something that should be disregarded as some minor inconvenience. She and her husband took their concerns to the Department of Health.
“We went to her [Sec. Jeanette Gain] and said, ‘this is something that we should be concerned about. We should start asking, why are they recommending this vaccine only for nine-year-olds and older because biologically it doesn’t make sense. What happens when you turn 10? There’s really not much difference if you’re ten or you’re eight, so why nine?’”
The week after the Dans spoke with Sec. Garin, they received a visit from a group of Sanofi’s scientists from France and Singapore who attempted to explain the company’s recommendations. Even then, the designation of 9 years old seemed arbitrary to Dans.
In May 2016, Halstead made his concerns known publicly when he sent a searing critique of WHO’s recommendation to The Journal of Infectious Diseases. In the paper, he notes that
Although the SAGE concluded that Dengvaxia can be safely administered to seronegative individuals aged >9 years, several lines of evidence suggest that Dengvaxia, when given to seronegative individuals of any age, permitted hospitalizations due to breakthrough DENV infection during year 3.
He argued that the combination of poor protection against circulating dengue virus strains and the presence of dengue antibodies satisfied the “known preconditions” for antibody-dependent enhancement of infections. Moreover, if that was the case, the usual methods of comparing vaccinated and placebo groups did not work.
Halstead continued to criticize SAGE by highlighting how they knew that “the greatest benefit would be expected in those who are seropositive at the time of vaccination” and insisted that there was “no rapid, point-of-care test” available that could indicate whether a person had been previously infected or not. According to him, tests were already available that would do just that.
He saved his sharpest attack for the same random age differentiation Dans took exception to. According to Halstead,
The report notes that ‘a statistically significant risk of hospitalized dengue was seen in (2-5 year old) vaccine recipients in the third year after the first dose’ but concluded simply that ‘this increased risk is currently not understood.’ Why not? The possibility that vaccine-enhanced disease occurred in individuals older and younger than 9 years old should have been subjected to careful scrutiny prior to vaccine licensure.
The pushback was not limited to members of the scientific community. In July 2016, Paulyn Ubial, then acting as secretary to Jeanette Garin, signed a resolution recommending that the immunization program be delayed due to insufficient data regarding the vaccine’s safety. She would later recall that subsequent to her suggestion, politicians pressured her to reverse.
"...during the budget hearing, there was a lot of pressure in Congress to expand it to other parts of the country with higher [cases] of dengue, which is Region 7. I didn’t give in to the pressure of Congress. I told them I cannot expand to other areas because of the recommendation of the expert panel," she said. "But I was pushed [and asked], 'Why can’t you have a second opinion?’" added Ubial.
Subsequently, she convened a second panel of experts. By this time, the World Health Organization had already published its first position on Dengvaxia that recommended the introduction of the dengue vaccine “only in geographic settings (national or subnational) where epidemiological data indicate a high burden of disease.”

On April 4, 2016, President Benigno Aquino III’s signature anti-dengue immunization program kicked off in earnest. Thousands of children across the National Capital Region in central Luzon spent a day of their summer vacation back in school for one reason: to receive their first dose of Sanofi’s Dengvaxia vaccine. The program would span presidential administrations. When all was said and done, almost a million children would have a partially effective vaccine coursing through their veins. In the eyes of some, it was a ticking time bomb.
During the time I’d spent in the Philippines, numerous people – all unknown to each other – would always declare in earnest and using the same exact words, “Life is hard here.” Day-to-day existence, for most families, was a tenuous undertaking with little wiggle room for mistakes or misfortune, whichever one bites first. For the children vaccinated with Dengvaxia and their helpless parents, life was about to get much harder through no fault of their own.
WORDS: Marc Landas.
IMAGE CREDIT: Malacañang Photo Bureau.



Leave a Reply